GettyImages
Nick Wilson, University of Otago; Amanda Kvalsvig, University of Otago, and Michael Baker, University of Otago
Despite a recent best-in-the-world ranking for its handling of COVID-19, New Zealand remains at risk as the pandemic intensifies globally. With more infectious variants of the virus emerging, there are many persisting concerns.
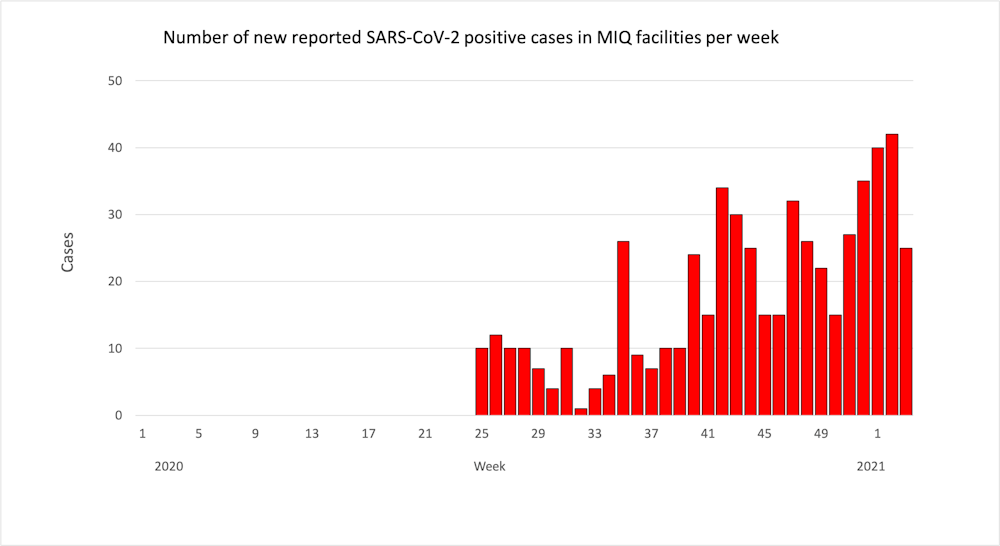
In particular, the number of infected people entering managed isolation and quarantine (MIQ) facilities at the border is increasing. This pressure contributes to the risk of border failures, which are now regular.
There have been at least nine since August 2020, including the most recent issues with the Pullman Hotel in Auckland.
We argue the time has come to “turn down the tap” of infected travellers coming from so-called “red zone” countries where the pandemic is out of control. We have already advocated for a traffic light system to achieve this.
One option is to reduce the risk of infected travellers getting on flights by using brief pre-departure quarantine and COVID-19 testing in carefully designed ways.
For example, an additional low-cost, rapid antigen test prior to boarding, plus clear instructions to passengers about the need for a period of pre-travel self-quarantine to reduce their risk of infection, could be a prerequisite.
A more intensive approach could require all red zone travellers to undergo pre-flight quarantine for five days in an approved airport hotel facility, with daily rapid (saliva) testing by New Zealand-certified officials.
The logistics of this could be simplified by having these approved airport hotel facilities located at specific travel hubs — for example, London, Hawaii and Singapore.
Another possibility is simply to further limit the bookings in MIQ facilities available to travellers from red zone countries — say, down to 500 travellers a month — to make the situation more manageable.
Australia has recently reduced the cap on incoming travellers. The New Zealand government could also temporarily suspend approval for any flights originating in red zone countries.
Of course, political decision-makers need to consider the immediate well-being of travellers coming from red zone countries (150 to 250 people per day on average).
Some are returning for compelling reasons: they have a health condition and genuinely fear dying in the pandemic, they are coming home to care for a sick relative, or they have lost a job overseas and lack financial support.
But these important considerations will apply to a relatively small number of individuals. They do not outweigh the far greater duty to the rest of New Zealand’s citizens to keep the country COVID-free.
Turning down the tap is important for maintaining COVID-19 elimination, providing multiple benefits:
Health authorities have a specific duty of care to protect workers in MIQ facilities from infection. While personal protective equipment (PPE) is provided, we know failures can still occur despite workers using it.
There is a case to be made that health authorities are currently not adequately meeting their duty of care by permitting large numbers of infected people to pass through these MIQ facilities.
Legal experts have considered the New Zealand Bill of Rights Act 1990, the Immigration Act 2009 and the International Covenant on Civil and Political Rights (OHCHR, to which New Zealand is a signatory) and confirmed the government can legally set conditions on returning NZ citizens — as is already being done.
There have been no successful legal challenges to New Zealand’s current quarantine requirements, or in Australia with its even tighter systems. Those requirements can logically be extended to include pre-flight quarantine and testing, and further limiting MIQ bookings to make border control safer and more manageable.
The claim that citizens are rendered “stateless” by such measures is a myth.
In summary, the risk of COVID-19 border control failures appears to be increasing. Action is needed to reduce the proportion of infected people boarding flights, or reducing travel from high-risk countries, or both.
There is no legal case against turning down the tap, provided it is clear such measures are time-limited and not absolute.
Nick Wilson, Professor of Public Health, University of Otago; Amanda Kvalsvig, Senior Research Fellow, Department of Public Health, University of Otago, and Michael Baker, Professor of Public Health, University of Otago
This article is republished from The Conversation under a Creative Commons license. Read the original article.
{kind=link}